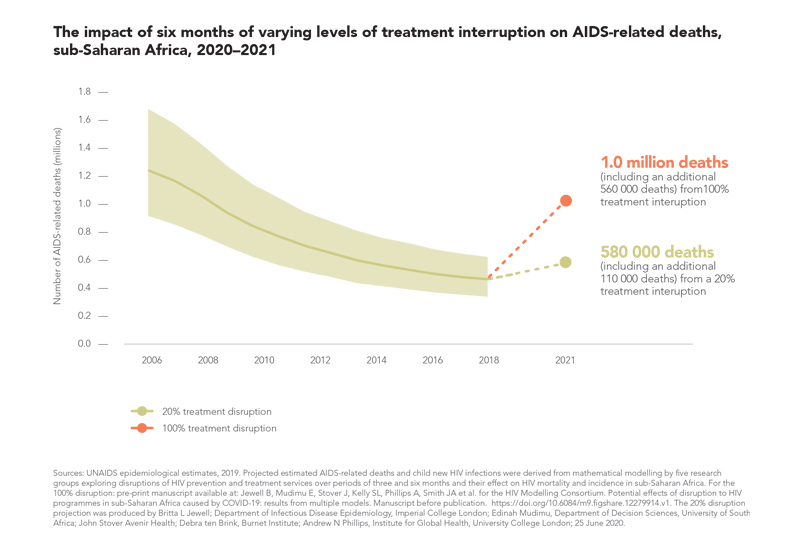
A six-month disruption in HIV treatment would cause more than
500 000 EXTRA deaths from AIDS-related illnesses in sub-Saharan Africa.
The Global Fund to Fight AIDS, Tuberculosis and Malaria has made up to US$ 1 BILLION available to help countries fight COVID-19.
AT LEAST 101 COUNTRIES have national policies for dispensing a three-month supply of medicine for people who are stable on antiretroviral therapy, and another 14 countries dispense a six-month supply for stable patients.
If current multimonth dispensing policies are fully implemented, an ESTIMATED 28% reduction in clinic visits could be achieved.
The COVID-19 pandemic is affecting the lives and livelihoods of people everywhere, but the impact is especially severe among people who are socioeconomically disadvantaged and marginalized, and among people with underlying medical conditions. As the coronavirus spreads in countries in sub-Saharan Africa with high HIV prevalence, there is evidence that people living with HIV and people with active tuberculosis are both at higher risk of COVID-related morbidity and mortality.
People living with HIV and people at higher risk of HIV infection are also facing life-threatening disruptions to health and HIV services as COVID-19 cases overwhelm health system capacities and lockdowns limit movement and strain economies. Voluntary medical male circumcision, condom production and distribution, pre-exposure prophylaxis (PrEP), HIV testing and treatment, and other programmes have all been negatively affected.
Recent modelling has estimated that a six-month disruption of antiretroviral therapy could lead to more than 500 000 [471 000–673 000] additional deaths from AIDS-related illnesses (including tuberculosis) in sub-Saharan Africa in 2020–2021. If services to prevent mother-to-child HIV transmission were similarly halted for six months, the estimated increases in new child infections would more than double in Malawi, Uganda and Zimbabwe, and increase by 83% in Mozambique.
A six-month total disruption in these services is an extreme scenario, but HIV service disruptions caused by lockdowns and the huge additional burden that COVID-19 has placed on health systems are very real. In the weeks prior to a partial lockdown in Zambia, for instance, a project funded by the United States President’s Emergency Plan for AIDS Relief (PEPFAR) that is providing antiretroviral therapy to almost 46 000 people living with HIV near military installations took special measures aimed at maintaining HIV testing and treatment services. This included strengthening the clinics’ patient communications approaches and safeguarding the logistics and supply chains for HIV medicines and test kits. As the partial lockdown began, the project nonetheless experienced steep drops in the number of HIV diagnoses, the number of people starting HIV treatment and the number of people living with HIV who were receiving their medications. The adjustments made before and during lockdown ultimately paid off, and services rebounded within a few weeks. However, they did not quite reach pre-crisis levels.

Similar scenarios playing out across countries and regions could see the global HIV response fall further behind on its 2020 commitments. For instance, if the COVID-19 pandemic interrupts antiretroviral therapy for 20% of people living with HIV for six months, it would result in more than 110 000 additional AIDS-related deaths.
HIV and other critical health services must be maintained as communities, cities and countries respond to this new pandemic. Countries around the world are accelerating HIV response innovations to minimize disruptions. At the same time, they are tapping into experience and investments from the HIV response, leveraging systems and applying lessons learned—lessons that stress the importance of political leadership, community engagement, rights-based and multisectoral approaches, and guiding actions with evidence.