Amid the upheaval associated with the COVID-19 pandemic, people-centred approaches pioneered by HIV programmes are demonstrating their ability to reach people with services, and they are being adopted more widely.
HIV service delivery models that emphasize client autonomy and self-care—and that minimize physical contact with health facilities—are critical during a time when health facilities need to manage the influx of COVID-19 patients, while at the same time maintaining vital health services without putting other clients at risk of COVID-19 infection.
HIV self-testing, which empowers people to choose for themselves the circumstances in which they take an HIV test, has the advantage of decongesting health facilities and increasing access to HIV testing to populations at higher risk of HIV infection. Burundi, Eswatini, Guatemala and Myanmar are among the countries that have reported expanding HIV self-testing during the COVID-19 pandemic.
The chairs in the HIV clinic waiting room at the Khmer–Soviet Friendship Hospital in the Cambodian capital, Phnom Penh, have been carefully placed a few metres apart from each other. The patients sitting in them wear face masks to prevent the spread of COVID-19. Behind a small reception desk are a group of women living with HIV who are part of the clinic’s essential staff—members of the Antiretroviral Users Association (AUA) who provide counselling, treatment literacy and support to people living with HIV.

Theary So is an AUA counsellor who has been living with HIV for 15 years. “I provide counselling services every day,” she says. “I did not stop coming to work even though I am scared that I might get infected with COVID-19.”
The Khmer–Soviet Friendship Hospital was the first HIV treatment site in Cambodia. Many years later, it is serving as the national COVID-19 centre, the country’s flagship facility fighting the new pandemic. Theary’s family worries about her continuing to work during the COVID-19 pandemic, but she soldiers on. “They all tell me to stop working in the antiretroviral therapy clinic. My children beg me to come home early.”
She takes precautions—including the use of face masks, gloves and alcohol sanitizer—to ensure she neither acquires nor transmits the new coronavirus to her patients, her family and her neighbours. That level of vigilance has helped Cambodia largely contain the spread of COVID-19: in early June 2020, there were 126 confirmed cases in the country and zero deaths.
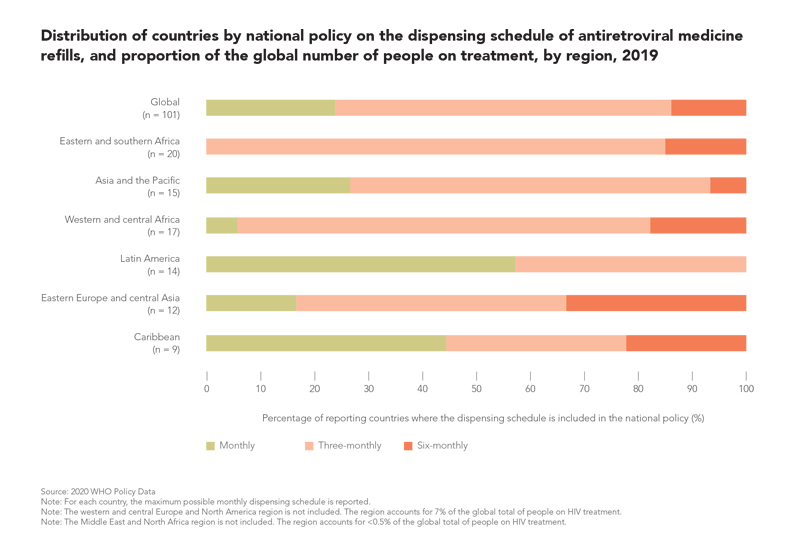
Crises are accelerators of innovation, and the COVID-19 crisis has accelerated a multitude of innovations as individuals, families, organizations and societies adapt to the new realities of social distancing and lockdown. HIV responses at the community, country and global level are no exception: more and more countries are shifting to multimonth prescription and dispensing of antiretroviral drugs so that people living with HIV are assured of uninterrupted supplies of their medications during the COVID-19 pandemic.
People-centred and differentiated approaches such as multimonth dispensing put people in charge of their HIV treatment, make health systems more adaptable and responsive, reduce the strain on standard health facilities, and free up those resources for other priorities. Multimonth dispensing does away with a patient’s need for frequent, costly and time-consuming clinic visits that are strictly to collect antiretroviral medications. It also reduces the workload of health-care facilities, and in the context of the COVID-19 crisis, it reduces the chances of acquiring the new coronavirus for both health-care workers and patients.
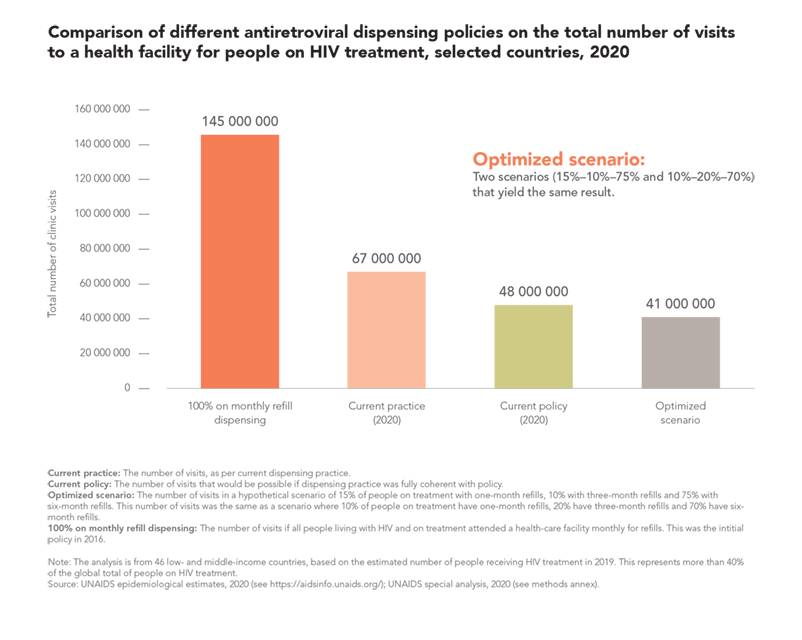
UNAIDS analysis of treatment data from 46 countries shows how implementation of multimonth dispensing policies has already more than halved the number of clinic visits, saving both time and money for health systems and people living with HIV. If current multimonth dispensing policies were fully implemented, an additional 28% reduction in clinic visits could be achieved, and an optimized scenario where 70% of people living with HIV on treatment in those countries are provided with a six-month supply of antiretroviral medicines would result in 26 million fewer antiretroviral medicine-related health facility visits per year, a 39% reduction.
UNAIDS has advised countries with sufficient stocks of antiretroviral medicines to switch to or extend multimonth dispensing, and to implement the necessary support services and systems (e.g., telephone or online adherence support and advice). In the context of the COVID-19 pandemic, multimonth dispensing should also be considered for other treatment programmes, including those for tuberculosis, viral hepatitis and various noncommunicable diseases, and for substitution therapy for opioid drug dependence. In Lesotho, for instance, tuberculosis patients can now receive three-month supplies of tuberculosis treatment.
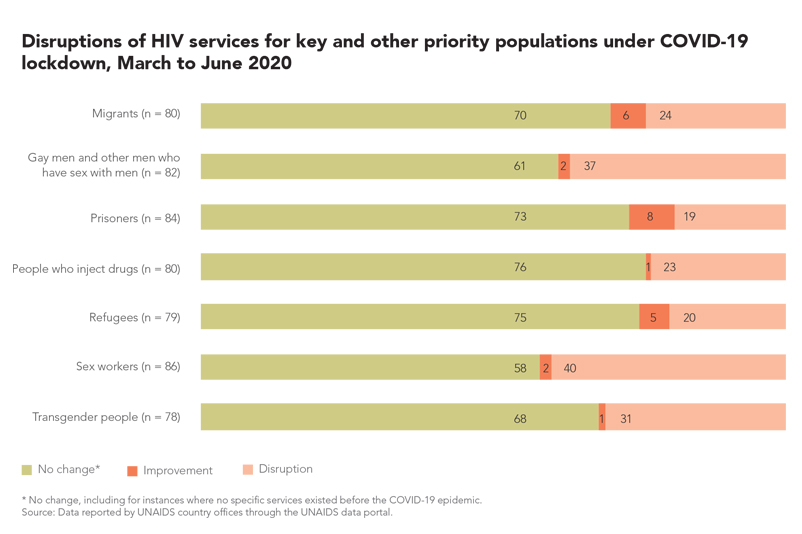
Key populations at higher risk of HIV infection already face a litany of challenges, and COVID-19 lockdowns have left them even more vulnerable than usual. Fears of contracting the novel coronavirus are compounded by the equally real danger of being exposed to aggressive enforcement of the lockdowns. There have been reports of sex workers and gay men and other men who have sex with men being scapegoated or harassed in Cameroon, Kenya, the Philippines, South Korea, Uganda and elsewhere. These challenges are creating even greater barriers to services for HIV and other health needs.