Integration involves delivering health services in complementary and coherent ways so that people get the care they need in ways that are effective, efficient and equitable.
Closer integration of HIV and other relevant health services has the potential to increase the reach and uptake of services, enhance efficiency, be cost-effective, make services more people-centred and improve their quality. Integrated services can better satisfy the intersecting health care needs of people than traditional, separated delivery models. As programme budgets come under increased pressure, the prospect of cost savings is also especially attractive to planners.
While there is good evidence that integration can have such positive effects, it is not always beneficial, and there can even be counterproductive results.
Integration can occur at multiple domains or levels.
Law and policy integration combines separate, disease-specific policies, strategies and plans to provide a unified structural framework and governance process, within which integrated services can be delivered. Such a high-level, unified policy framework can guide service providers and make clear the need for them to act in a unified, holistic and comprehensive manner.
Systems linkages can establish unified support systems that facilitate and enable delivery of integrated services. Linked systems include health worker education and training, procurement and supply chain management, pharmacy and laboratory services, health management information and client management systems, and integrated budgeting. This can enhance coordination and support more streamlined and efficient services.
Service integration can range from linking certain services or adding them to specialized platforms, to fully integrating services in one location (so-called one-stop shops). Integration can also occur at different levels.
Full service-level integration has many advantages for health-care users. When clinical services (e.g., for HIV and tuberculosis, or for HIV and sexual and reproductive health) are integrated, it can favour people-centred approaches. But this level of integration can also involve trade-offs with respect to staff workloads, the quality of care and the provision of tailored services, and human rights violations such as discrimination and breeches of confidentiality also can occur. Finally, it can be challenging and expensive to bring the necessary services together in a single place.
Multifacility integration involves networking health facilities and other service providers so that people with complex problems can conveniently access specialist care. Coordination can be difficult, though. Another model involves a case manager overseeing care and referring patients to specialists, as needed. This requires highly skilled case managers, who may be difficult to recruit and retain in health systems that are facing health worker shortages.
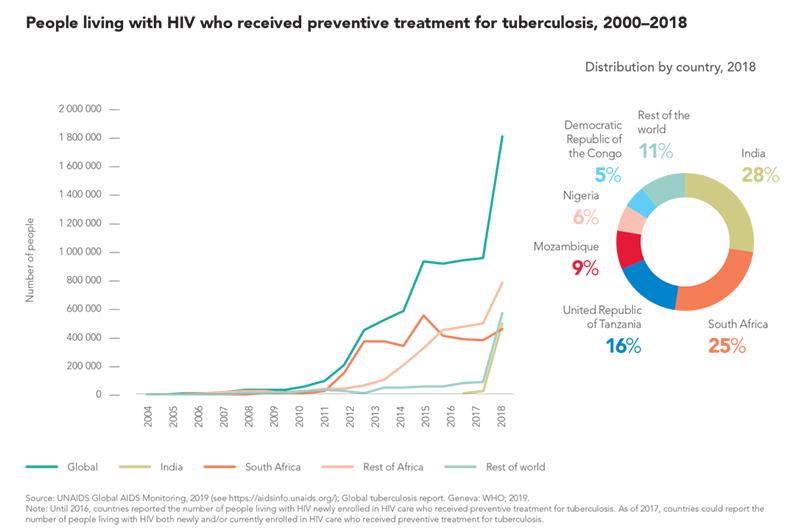
Tuberculosis is one of the top 10 causes of death worldwide and the leading cause of death among people living with HIV (see Chapter 2). Preventive treatment for tuberculosis among people living with HIV in 65 high-burden countries has improved dramatically in recent years, reaching 1.8 million in 2018.
Despite this progress, large gaps in tuberculosis detection and preventive treatment exist in several high-burden countries. In 66 countries with available data, coverage of tuberculosis preventive treatment among people living with HIV who were newly enrolled in care was just 49% in 2018. Among the 11 high TB/HIV burden countries that reported these data, coverage ranged from 10% in Indonesia to 97% in the Russian Federation. About 0.8 million of the 10 million new tuberculosis cases globally in 2018 were among people living with HIV.
Integrating tuberculosis and HIV services is therefore vitally important for the control of both diseases. Among 30 countries with high burdens of both HIV and tuberculosis, 11 reported having countrywide (i.e., greater than 95% of health facilities providing HIV treatment and care) colocation of services providing HIV testing with WHO-recommended rapid molecular tuberculosis diagnostics; just five reported that both antiretroviral therapy and tuberculosis treatment are provided in the same health facility countrywide.
Deeper integration can be difficult in poorly resourced health systems. Facilities may lack staff with sufficient training to provide integrated care, and they may not be equipped to provide the prompt tuberculosis screening and testing that is required. Study evidence from South Africa, Uganda and Zambia show that such hurdles can be overcome, with success requiring the management of potential increases in staff workload, dealing with record-keeping challenges and maintaining effective infection control. Strong and supportive management is especially important, as shown in a recent review from South Africa.